EMDR Treatment Effectiveness: What the Research Shows

TL;DR:
EMDR therapy is a structured, evidence-based approach that effectively reduces PTSD, trauma, anxiety, and depression symptoms. Its success depends on treatment intensity, the therapist-client relationship, and personalized care, with most clients noticing improvements within six sessions. Combining EMDR with personalized scheduling and strong therapeutic alliances enhances long-term recovery outcomes.
Eye Movement Desensitization and Reprocessing (EMDR) therapy is defined as a structured, evidence-based treatment that produces measurable reductions in PTSD, trauma, anxiety, and depression symptoms through guided bilateral stimulation and memory reprocessing. EMDR treatment effectiveness is now supported by decades of clinical trials, and the World Health Organization, the American Psychiatric Association, and the U.S. Department of Veterans Affairs all formally endorse it as a first-line intervention for PTSD. A 2026 randomized trial reported an effect size of Cohen's d ≈ 1.88 for core PTSD symptom reduction, placing EMDR among the most potent psychological treatments available. If you are living with trauma, PTSD, or anxiety and wondering whether therapy can actually move the needle, the clinical evidence gives a clear answer.
What does research say about EMDR treatment effectiveness for PTSD?
EMDR produces large, clinically significant reductions in PTSD symptoms. A 2026 randomized controlled trial found effect sizes of Cohen's d ≈ 1.88 compared to passive controls, with measurable improvements appearing by mid-treatment and continuing through 12 sessions. An effect size that large means the average person receiving EMDR improved more than roughly 97% of those who received no treatment. That is not a marginal benefit. It is a substantial shift in daily functioning.
The trial also confirmed that PTSD symptoms do not improve spontaneously after crisis events without structured psychological intervention. Waiting it out is not a strategy. Without treatment, symptoms tend to persist or worsen, which makes early engagement with a structured protocol like EMDR especially important.
EMDR's eight-phase protocol targets the specific traumatic memories driving symptoms rather than managing surface-level distress. Phases include history-taking, preparation, assessment, desensitization, installation, body scan, closure, and reevaluation. Each phase builds on the last, which is why consistent attendance matters so much for lasting PTSD recovery.
| Measure | EMDR Result | Comparison |
|---|---|---|
| Core PTSD symptom effect size | Cohen’s d ≈ 1.88 | Passive control |
| Symptom improvement onset | Mid-treatment (by session 6) | Baseline |
| Continued improvement | Post-treatment follow-up | End of active sessions |
| Endorsing organizations | WHO, APA, VA | N/A |
Pro Tip: Track your symptom severity before and after each session using a simple 0–10 distress rating. Seeing your own numbers drop over time reinforces that the process is working, even on weeks when progress feels invisible.
How effective is EMDR for anxiety and depression related to trauma?
EMDR's benefits extend well beyond PTSD. A meta-analysis of 40 randomized controlled trials found that EMDR produced significant symptom reductions in both anxiety and depression, with a standardized mean difference of -1.10 compared to passive controls. A standardized mean difference of that magnitude is considered large in clinical psychology. It means EMDR moves the needle on mood and anxiety in ways that are statistically and practically meaningful.
Anxiety reductions were slightly larger than depression reductions across the studies. This makes clinical sense. EMDR directly targets the fear-based memory networks that drive hypervigilance, avoidance, and panic, which are the core mechanisms of anxiety. Depression linked to trauma often involves more complex cognitive patterns, so the effect, while still significant, is somewhat smaller.
EMDR also helps people who carry trauma-related distress that does not meet the full diagnostic threshold for PTSD. Trauma events that disrupt daily life but fall short of a formal PTSD diagnosis still respond to EMDR's reprocessing approach. This broadens who can benefit considerably.
Key findings on EMDR for anxiety and depression:
Standardized mean difference of -1.10 versus passive controls across 40 RCTs, indicating large overall effect.
Anxiety reductions were slightly larger than depression reductions, consistent with EMDR's mechanism of targeting fear-based memory networks.
Study heterogeneity exists across the 40 trials, meaning individual results vary based on trauma type, severity, and treatment delivery.
Sub-threshold trauma responds to EMDR even when a full PTSD diagnosis is not present.
Pro Tip: If you are managing both anxiety and depression alongside trauma, tell your therapist which symptoms feel most disabling right now. EMDR can be sequenced to prioritize the memories most connected to your current distress.
What factors influence EMDR success and completion rates?
Treatment completion is one of the strongest predictors of good outcomes. Across 73 studies of trauma-focused interventions, the average completion rate was 71.8%, with higher-intensity schedules linked to better completion and outcomes. That figure tells a clear story: people who finish treatment do better, and the structure of treatment affects whether they finish.
Two factors independently predict how much PTSD symptoms improve during EMDR: treatment intensity and therapeutic alliance. Treatment intensity predicts improvement throughout the entire course of therapy, while the therapeutic alliance becomes especially important after the midpoint of treatment. Early gains come from the structured protocol itself. Sustained gains depend on the relationship between you and your therapist.
Personalizing session frequency and total session count also matters. Rigid session counts do not serve every person equally. Tailoring intensity to individual needs reduces premature dropout and improves clinical outcomes. Some people benefit from weekly sessions over several months. Others respond better to EMDR Intensives, which compress treatment into fewer, longer sessions over a shorter period. The advantages of EMDR intensives include faster symptom relief and fewer scheduling barriers for people with demanding lives.
Practical factors that maximize your EMDR outcomes:
Consistent attendance prevents momentum loss between sessions and supports the cumulative reprocessing effect.
Open communication with your therapist about distress levels between sessions allows for real-time treatment adjustments.
Flexible scheduling through intensive formats can improve completion for people who struggle with weekly appointments.
Therapeutic trust built over the first half of treatment becomes the foundation for the deeper work in later sessions.
Pro Tip: If you feel stuck or like sessions are not progressing, say so directly. Adjusting session frequency or format is a clinical tool, not a sign of failure.
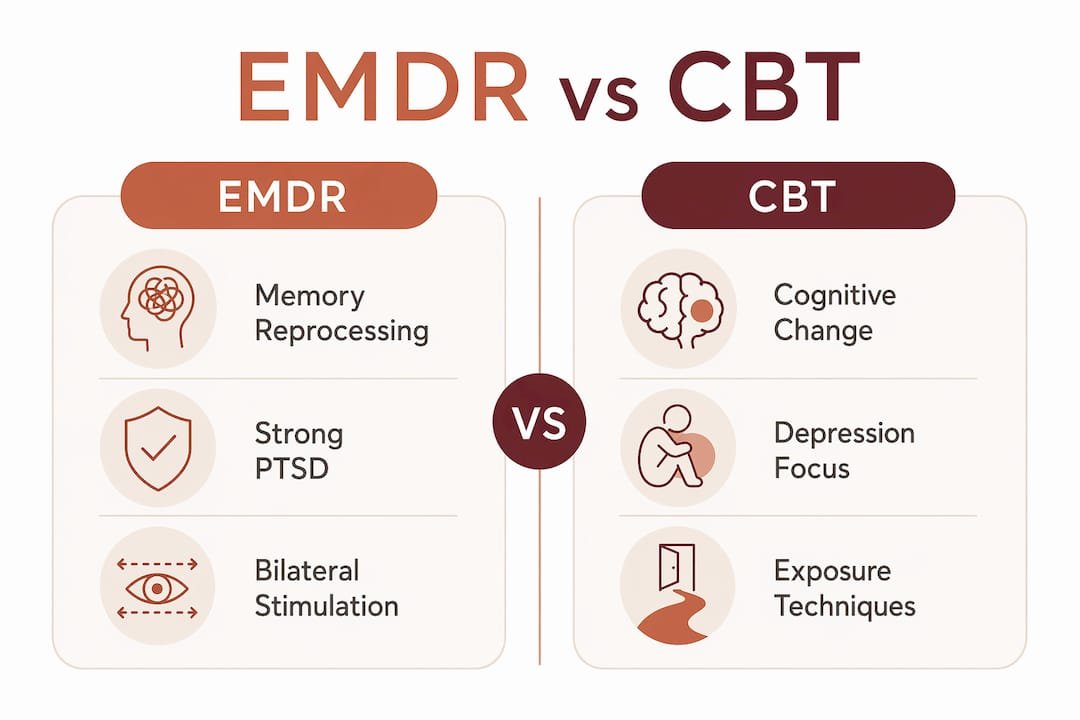
How does EMDR compare with CBT for trauma treatment?
EMDR and Cognitive Behavioral Therapy (CBT) both produce large reductions in PTSD symptoms, and the clinical evidence does not declare one categorically superior. The 2026 randomized trial found comparable overall efficacy between the two approaches, with combined effect sizes of approximately d = 1.9 for PTSD and d = 1.4 for depression. The difference lies in what each therapy targets most directly.
EMDR focuses on reprocessing the traumatic memory itself. It works by reducing the emotional charge attached to specific memories through bilateral stimulation, typically eye movements, taps, or tones. CBT, particularly Trauma-Focused CBT, works through cognitive restructuring and behavioral activation. It challenges the distorted beliefs that trauma creates and builds new behavioral patterns. These are different mechanisms aimed at overlapping problems.
EMDR tends to produce stronger reductions in core PTSD symptoms, while CBT shows stronger effects on depressive symptoms. This is not a competition. For many people, the two approaches are genuinely complementary. A therapist might use EMDR to process a specific traumatic event and then use cognitive techniques to address the beliefs that event created. Understanding how EMDR differs from talk therapy helps you make an informed choice about which path fits your situation.
| Feature | EMDR | Trauma-Focused CBT |
|---|---|---|
| Primary mechanism | Bilateral stimulation, memory reprocessing | Cognitive restructuring, behavioral activation |
| Strongest effect | Core PTSD symptom reduction | Depressive symptom reduction |
| Requires verbal processing | Minimal verbal narration of trauma | Detailed verbal engagement with trauma content |
| Session structure | Highly structured 8-phase protocol | Structured but more flexible across models |
| Best combined with | CBT for cognitive distortions | EMDR for direct memory processing |
Pro Tip: Ask your therapist whether they integrate EMDR and CBT techniques. Many licensed trauma therapists use both within the same treatment plan, which the research supports as a sound clinical approach.
What should you expect from EMDR treatment in practice?
EMDR therapy follows a predictable arc, even though the emotional experience varies from person to person. Benefits often begin by mid-treatment and continue to build after the active treatment phase ends. Knowing this timeline helps you stay committed during early sessions when progress can feel slow.
A standard course of EMDR typically unfolds as follows:
Sessions 1–3 (History and preparation): Your therapist gathers your trauma history, explains the protocol, and teaches stabilization skills. No active reprocessing happens yet.
Sessions 4–6 (Assessment and desensitization): Reprocessing begins. You identify target memories and work through them using bilateral stimulation. Distress levels often spike briefly before dropping.
Sessions 7–9 (Installation and body scan): Positive beliefs replace negative ones. Your therapist checks for residual physical tension connected to the memory.
Sessions 10–12 (Closure and reevaluation): Progress is reviewed. Remaining targets are identified. Many people notice continued improvement between sessions during this phase.
Post-treatment: Symptom scores continue to decrease after the final session for most people, which reflects the ongoing nature of memory consolidation.
Consistent attendance across all phases is what separates people who see lasting change from those who plateau. EMDR for trauma works best when you treat each session as a building block, not a standalone event.
Key Takeaways
EMDR therapy produces large, clinically validated reductions in PTSD, anxiety, and depression, with the strongest outcomes driven by treatment intensity, therapeutic alliance, and personalized session planning.
| Point | Details |
|---|---|
| Large effect on PTSD | A 2026 trial found Cohen’s d ≈ 1.88, placing EMDR among the most effective psychological treatments. |
| Broad symptom coverage | EMDR reduces anxiety and depression significantly, not just PTSD, with an SMD of -1.10 across 40 RCTs. |
| Completion drives outcomes | The average completion rate across trauma studies is 71.8%; finishing treatment is strongly linked to better results. |
| Alliance matters most later | Therapeutic alliance predicts sustained improvement after mid-treatment, making the therapist relationship a clinical tool. |
| Personalization beats rigid protocols | Tailoring session frequency and intensity to individual needs reduces dropout and improves clinical outcomes. |
What most people miss about EMDR
The conversation around EMDR tends to focus on the bilateral stimulation, the eye movements, the tapping, as if that mechanism is the whole story. After working closely with trauma-informed care and reviewing the clinical literature, I think that framing misses the most important variable: the relationship between client and therapist, and the sustained commitment to completing treatment.
Early symptom relief in EMDR is real. People often feel measurable improvement within the first several sessions, and that early progress is driven largely by the structured protocol itself. But the research is clear that sustained recovery depends on what happens after that initial phase. Therapeutic alliance becomes the dominant predictor of improvement in the second half of treatment. That means the trust you build with your therapist is not just a comfort. It is a clinical mechanism.
The other thing most articles skip is the dropout problem. A completion rate of 71.8% means roughly one in four people does not finish. Intensive formats and personalized scheduling exist specifically to address this. If weekly appointments feel like too much of a barrier, that is a clinical conversation worth having, not a reason to delay treatment.
EMDR is not a quick fix, and it is not magic. It is a well-validated process that requires your active participation and a therapist who knows how to adjust the approach to your needs. The evidence is strong. The outcomes are real. The work is yours to do.
— Juiced
Alvaradotherapy's approach to evidence-based EMDR care
Alvaradotherapy brings the clinical rigor behind EMDR research directly into its practice, serving adults across California who are ready to address trauma, PTSD, and anxiety with a structured, personalized approach.

The licensed therapists at Alvaradotherapy tailor session intensity and format to each person's needs, including EMDR Intensives for those who want faster progress or have scheduling constraints. Services are available online throughout California, with bilingual support in English and Spanish. If you are ready to understand what the process actually looks like, the what to expect page walks you through each phase of treatment clearly. For those dealing specifically with PTSD or complex trauma, Alvaradotherapy's PTSD and complex trauma services offer targeted, evidence-aligned care built around your history and goals.
FAQ
What is EMDR treatment effectiveness based on?
EMDR treatment effectiveness is based on randomized controlled trials and meta-analyses showing large reductions in PTSD, anxiety, and depression symptoms. A 2026 trial reported an effect size of Cohen's d ≈ 1.88 for core PTSD symptoms compared to passive controls.
How many EMDR sessions does it take to see results?
Most people begin noticing measurable symptom improvement by mid-treatment, typically around sessions 4–6. Improvements continue after the active treatment phase ends, making session completion a key factor in lasting recovery.
Does EMDR work for anxiety and depression, not just PTSD?
Yes. A meta-analysis of 40 randomized controlled trials found EMDR produces significant reductions in both anxiety and depression, with a standardized mean difference of -1.10 compared to passive controls. Anxiety reductions were slightly larger than depression reductions.
Is EMDR or CBT better for trauma treatment?
Neither is categorically superior. EMDR produces stronger reductions in core PTSD symptoms, while CBT shows stronger effects on depressive symptoms. The two approaches are complementary and are often used together within a single treatment plan.
What affects whether EMDR therapy works?
Treatment intensity, therapeutic alliance, and consistent attendance are the three strongest predictors of EMDR outcomes. Personalizing session frequency to individual needs also reduces dropout and improves clinical results.
Recommended
EMDR Therapy for Trauma: Steps, Effectiveness & Help in California — Alvarado Therapy
EMDR and Relationships: Healing Trauma for Deeper Connection — Alvarado Therapy
EMDR Intensives for Trauma: 70% Faster Healing Results — Alvarado Therapy
EMDR Therapy in PTSD Recovery: Lasting Change and Hope — Alvarado Therapy