Workflow for Trauma-Informed Care: A Clinical Guide
TL;DR:
A trauma-informed care workflow systemically applies SAMHSA's six core principles at every client contact point, transforming clinical practice. It involves specific stages, protocols, and written procedures to ensure consistent, trauma-sensitive responses that reduce retraumatization and improve engagement. Embedding these principles organizationally sustains long-term trauma-informed practice, benefiting both clients and staff through ongoing evaluation and clear operational standards.
A trauma-informed care workflow is a structured clinical and organizational process that applies SAMHSA's six core principles — safety, trustworthiness, peer support, collaboration, empowerment, and cultural sensitivity — at every point of client contact. This is not a philosophy layered on top of existing practice. It is a redesign of how care gets delivered, documented, and sustained. When mental health professionals and caregivers build these principles into each stage of service, from intake through discharge, they reduce retraumatization, improve treatment engagement, and create conditions where healing becomes possible. This guide breaks down the exact steps, tools, and organizational strategies that make that happen.
What is the workflow for trauma-informed care?
A trauma-informed care workflow is a sequence of clinical and organizational steps that embed trauma knowledge into every policy, interaction, and decision point. SAMHSA defines a trauma-informed organization as one that recognizes trauma's widespread impact, identifies trauma signs in clients and staff, and responds by integrating that knowledge across all practices. That definition has direct workflow implications. It means the workflow is not just a clinical checklist. It is a system-level commitment.
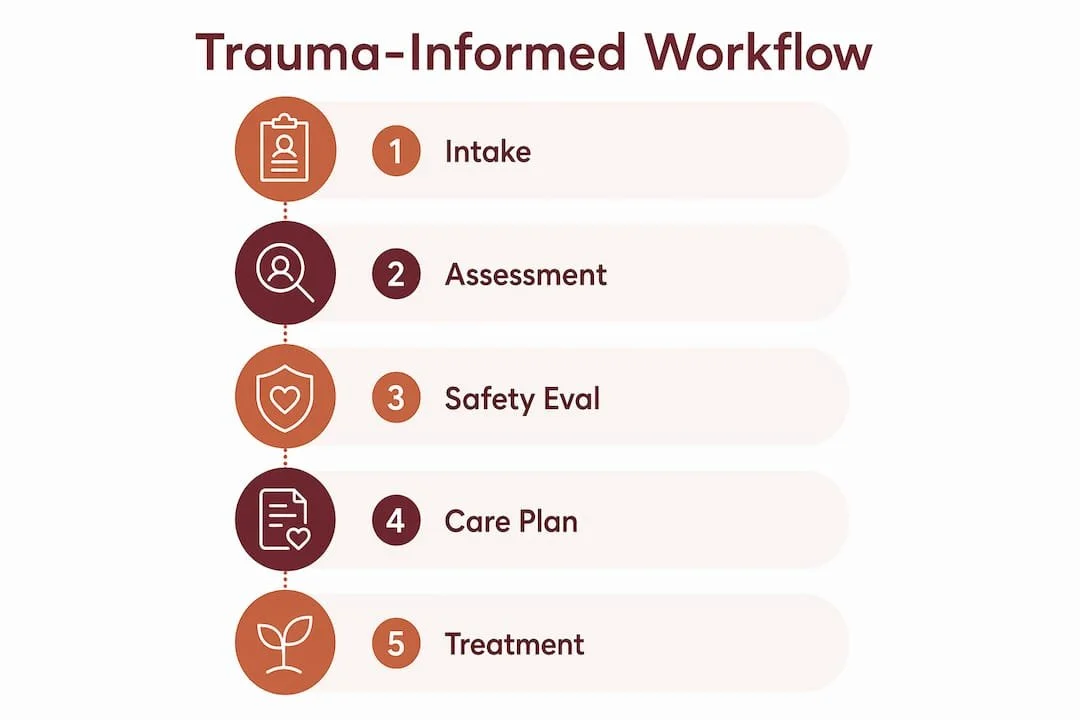
The standard workflow moves through seven core stages:
Intake and screening — Administer a validated trauma screening instrument at first contact.
Assessment — Conduct a structured trauma assessment that maps history, symptoms, and risk factors.
Safety and risk evaluation — Screen for suicide risk and immediate safety concerns with defined action protocols.
Care planning — Develop a collaborative plan that reflects client goals and cultural context.
Treatment and intervention — Deliver evidence-based trauma therapies with ongoing client feedback loops.
Documentation — Record in trauma-sensitive language that avoids pathologizing or retraumatizing.
Referral and crisis response — Activate warm handoffs and clear escalation pathways when needed.
Each stage maps directly to SAMHSA's six principles. Intake reflects trustworthiness and transparency. Care planning reflects collaboration and mutuality. Referral protocols reflect safety. The CPM-PTS model from the National Children's Alliance demonstrates this in pediatric settings, using a 15-item validated screening tool paired with structured safety planning and referral pathways. That pairing is the key design insight: screening without a defined next step is not a workflow. It is a missed opportunity.
Organizations that want to build this at the system level benefit from a four-phase change structure: plan, assess, implement, and sustain. The Trauma-Informed Organizational Change Manual from the Trauma-Informed Network Resource Center provides toolkits and self-assessments for each phase. This structure prevents the most common failure mode, which is training staff on trauma principles without ever converting those principles into written operational procedures.

How do you operationalize this workflow in clinical encounters?
Clinical operationalization means converting principles into specific behaviors during actual client visits. The shift from "what's wrong with you?" to "what happened to you?" described by Rutgers Brandt Center is the foundational stance change. That shift shapes every interaction, from how you open a session to how you document a client's history.
Here is what that looks like in practice during a clinical encounter:
Use validated screening tools at intake. The CPM-PTS 15-item screener is one example. Tools like the ACE questionnaire, the PC-PTSD-5, or the Child Trauma Screening Questionnaire each serve different populations. The tool matters less than the commitment to screen consistently and act on results.
Communicate transparently at every step. Tell clients what you are doing, why you are doing it, and what happens next. Opaque processes recreate the powerlessness that trauma survivors have already experienced.
Conduct safety and suicide risk assessments with clear protocols. Every clinician on your team needs to know exactly what to do when a screen is positive. That means written decision rules, not individual judgment calls.
Document in trauma-sensitive language. Avoid language that implies blame, pathology, or character deficiency. Phrases like "client reports difficulty regulating emotions" are more accurate and less harmful than "client is manipulative."
Build shared decision-making into care planning. Clients who actively participate in their care show better treatment engagement and reduced dropout rates. Give clients real choices about treatment modalities, session frequency, and goal priorities.
Pro Tip: Before any new screening protocol goes live, map the full referral pathway first. If a client screens positive for PTSD and your practice has no defined next step, you have created a clinical dead end. The CPM-PTS model specifies who acts, what outputs are expected, and what happens before the client leaves the building. That level of specificity is the standard to aim for.
For a deeper look at conducting structured trauma assessments, Alvaradotherapy's guide on trauma assessment practices walks through the clinical steps in detail.
How do you embed trauma-informed workflows into organizational culture?
Individual clinician skill is necessary but not sufficient. Trauma-informed care is a systemic integration into policies and practices, not just individual empathy. That distinction matters enormously for organizational leaders. You can have a staff of highly empathic clinicians and still deliver care that retraumatizes clients if your intake forms, documentation systems, and referral processes are not designed with trauma in mind.
The organizational workflow has four phases:
Plan: Define your trauma-informed care goals, identify champions, and secure leadership commitment. Without executive support, workflow changes stall at the pilot stage.
Assess: Use formal self-assessment tools to evaluate current policies, physical environments, and staff practices. The Trauma-Informed Organizational Change Manual includes structured instruments for this phase.
Implement: Translate principles into written decision rules. Specify screening protocols, documentation standards, referral procedures, and crisis response steps. Train all staff, including administrative and support staff, not just clinicians.
Sustain: Build continuous evaluation into the workflow itself. Review outcomes data quarterly, gather client feedback, and adjust protocols based on what you find.
Pro Tip: Administrative staff are often the first point of contact for trauma-affected clients. A front desk team that does not understand trauma principles can undermine everything a clinician does in the session. Include reception, billing, and intake coordinators in all trauma-informed training.
| Organizational Phase | Key Activity | Primary Output |
|---|---|---|
| Plan | Leadership alignment and goal setting | Written trauma-informed care commitment statement |
| Assess | Organizational self-assessment | Gap analysis and readiness report |
| Implement | Policy and procedure development | Written protocols for screening, documentation, referral |
| Sustain | Ongoing evaluation and feedback loops | Quarterly outcome reviews and protocol updates |
Many institutions train staff on trauma principles but fail to translate that training into operational decision rules. The result is a knowledge gap that shows up as inconsistent screening, unclear referral processes, and documentation that inadvertently retraumatizes clients. Written protocols close that gap.
What are the most common workflow failures and how do you fix them?
Workflow failures in trauma-informed care are predictable. Most fall into four categories, and each has a direct fix.
Screening without action pathways. A positive trauma screen with no defined next step leaves both the client and the clinician in an unresolved state. Fix: Write explicit decision rules before launching any screening protocol. Define who receives the result, what the response options are, and how the client is informed.
Opaque documentation practices. Notes written in clinical shorthand or deficit-focused language can retraumatize clients who access their own records. Fix: Adopt a documentation standard that uses descriptive, non-judgmental language and reflects the client's own words where appropriate.
Warm handoffs that are not warm. Referring a client to another provider without a direct introduction or a clear explanation of why creates a gap that trauma-affected clients often do not cross. Fix: Build warm handoff protocols into your referral workflow. This means a direct introduction, a shared care summary, and a follow-up check-in.
Staff burnout and secondary trauma. Clinicians who carry unaddressed vicarious trauma deliver less consistent care. Fix: Build resistance to retraumatization checkpoints into staff supervision, including regular debriefs, peer consultation, and explicit workload limits.
The CPM-PTS model addresses the first failure directly by requiring that every workflow step specify who acts, what the expected output is, and what the next step is before the client leaves. Treating your workflow as a touchpoint map, where every client interaction has a responsible actor and a defined output, prevents most of these failures before they occur.
Alvaradotherapy's resource on trauma recovery workflows offers additional frameworks for building these safeguards into everyday practice.
Key takeaways
An effective workflow for trauma-informed care requires converting SAMHSA's six principles into written clinical protocols, organizational policies, and staff practices at every point of client contact.
| Point | Details |
|---|---|
| Start with SAMHSA’s framework | Map all six core principles to specific workflow stages before designing any protocol. |
| Screen with defined next steps | Pair every validated screening tool with explicit action pathways before the client leaves. |
| Translate training into written rules | Staff knowledge alone does not prevent retraumatization. Written decision rules do. |
| Include all staff, not just clinicians | Administrative and support staff shape the client experience before any session begins. |
| Build in continuous evaluation | Quarterly outcome reviews and client feedback loops keep workflows accurate and effective. |
What i've learned designing trauma-informed workflows
The most persistent mistake I see in clinical settings is treating trauma-informed care as a training event rather than a workflow redesign. Organizations send their staff to a two-day workshop, check the box, and expect practice to change. It does not. What changes practice is a written protocol that tells a clinician exactly what to do at 3:00 PM on a Tuesday when a client screens positive and the referring provider is unavailable.
The question shift from "what's wrong with you?" to "what happened to you?" sounds simple. In practice, it requires rewriting intake forms, retraining documentation habits, and redesigning how supervisors give feedback. That is organizational change work, not just clinical sensitivity work.
The practices that sustain trauma-informed workflows long-term share one feature: they treat staff well-being as a workflow variable, not a personal responsibility. When secondary trauma is addressed through supervision structures and peer consultation, clinicians stay consistent. When it is ignored, workflows degrade quietly until a crisis makes the gap visible.
The benefits of trauma-informed care show up most clearly in settings where the workflow is explicit, the protocols are written, and leadership treats the model as a system commitment rather than a clinical preference.
— Juiced
Trauma therapy that puts these principles into practice
If you are a client looking for care that actually operates this way, Alvaradotherapy in California builds these workflow principles into every service it offers.
Alvaradotherapy's licensed therapists deliver EMDR trauma therapy and PTSD and complex trauma treatment using structured, trauma-sensitive workflows that prioritize your safety, transparency, and active participation at every step. Services are available in English and Spanish, online across California, and in person in Pasadena and Ventura. If you are ready to work with a practice that treats trauma-informed care as a system commitment rather than a tagline, book a consultation to get started.
FAQ
What is meant by trauma-informed care in clinical practice?
Trauma-informed care is a clinical and organizational approach that recognizes trauma's widespread impact and integrates that knowledge into all policies, practices, and interactions. SAMHSA defines it through six core principles: safety, trustworthiness, peer support, collaboration, empowerment, and cultural sensitivity.
Why is a structured workflow necessary for trauma-informed care?
A structured workflow converts trauma-informed principles into specific, repeatable clinical actions. Without written protocols for screening, documentation, and referral, care becomes inconsistent and risks retraumatizing the clients it is meant to support.
What are the steps for trauma-informed care in a clinical workflow?
The core steps are intake screening, structured assessment, safety and risk evaluation, collaborative care planning, evidence-based treatment, trauma-sensitive documentation, and warm handoff referrals. Each step should specify who acts, what the output is, and what happens next.
What is the role of trauma-informed care in organizational settings?
At the organizational level, trauma-informed care requires embedding trauma principles into hiring practices, physical environments, supervision structures, and written policies. Individual clinician skill without organizational support produces inconsistent outcomes.
What are the benefits of trauma-informed care for clients and staff?
Clients experience greater safety, transparency, and treatment engagement. Staff benefit from reduced secondary trauma when supervision and peer consultation are built into the workflow as standard practice rather than optional resources.